Intracranial EEG Epilepsy - Study 5
Data for a patient with epilepsy obtained for clinical treatment and collected for research, consisting of a large left-sided intracranial EEG dataset (grid, strip, and depth electrodes) with multiple seizures.
Dataset Overview
This patient is a right-handed, 16-year old male who was admitted to the epilepsy monitoring unit for intracranial monitoring. The age of onset was 1 year old.
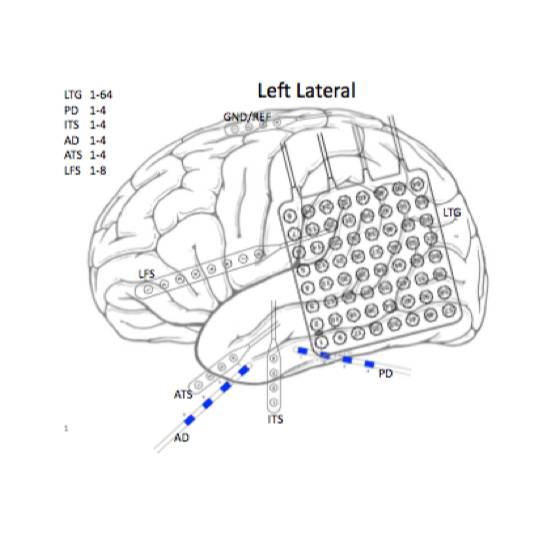
These data are from an 8-contact straight strip inserted into the left frontal region parallel to the superior temporal gyrus, an 8x8 grid inserted over the left posterior temporo-occipital region, a 4-contact straight strip inserted over the left anterior temporal pole, a 4-contact straight strip inserted over the left inferior subtemporal region, posterior to the anterior temporal strip, a 4-contact orthogonal depth electrode inserted between the anterior temporal strip and inferior subtemporal strip, targeting the hippocampus, and another 4-contact orthogonal depth electrode targeting the hippocampus.
This is an abnormal computer-assisted prolonged intracranial EEG monitoring session, lasting approximately 2 days, due to the presence of frequent independent left posterior temporo-occipital, left mesial temporal and left anterior temporal epileptiform discharges. During the monitoring session, the patient had four complex partial seizures. All of these seizures began in the posterior contacts of the left temporo-occipital grid. The findings would be consistent with a localization-related epilepsy with seizure onset in the left occipital neocortex. The patient underwent a surgery for reopening of left tempooccipital craniotomy, removal of subdural grids and depth electrodes, and left occipital pole resection. Pathology samples for cortex and underlying white matter with changes consistent with remote destructive injury. The cortex shows multiple areas of severe neuronal loss and gliosis associated with atrophy and focal dystrophic calcification. Calcifications are present focally in the meninges and vascular walls. An immunohistochemical stain was performed on paraffin-embedded tissue using antibodies to GFAP. GFAP highlights disruption of the normal cortical architecture, reactive gliosis and subpial gliosis. An immunohistochemical stain for NeuN highlights neurons. GROSS DESCRIPTION: Received fresh labeled "left occipital brain lobe" is a 7.51 gram, 5.2 x 2.8 x 0.8 cm portion of brain. The specimen is sent in formalin to the neuropathology working group for sectioning.
46-month post-resection ILAE 1 outcome score
Files
1 - 0 of 0 files
About this dataset
Publishing history
Cite this dataset
Tags
Copyright © 2026 University of Pennsylvania. All rights reserved.